krsct
GLP-1 Apprentice
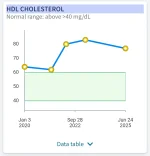
Been on GLP-1 for almost 3 years. Lost 1/4 of body weight in 8 months and maintenance since then. Took a while but my doctor stopped my statins today. Never thought it would happen. It took a while but another great NSV.

That is awesome, keep us posted to see if the cholesterol numbers creep back up.Been on GLP-1 for almost 3 years. Lost 1/4 of body weight in 8 months and maintenance since then. Took a while but my doctor stopped my statins today. Never thought it would happen. It took a while but another great NSV.
I'm at 90. My doc does not think that 55 is reasonable. Will also reassess in 6 months.Congrats. What cholesterol numbers did you hit? The new <55 mg/dL LDL targets are tough.
FAREFFINOUTBeen on GLP-1 for almost 3 years. Lost 1/4 of body weight in 8 months and maintenance since then. Took a while but my doctor stopped my statins today. Never thought it would happen. It took a while but another great NSV.
Agree with this, coronary calcium score is a very good way to determine if statins are needed or not, and is especially useful where calculated risk based on family history, blood pressure , lipids, blood sugar, smoking etc is intermediate, and it will still show changes if those numbers are improved by weight loss, and treatment is an extremely good idea if CCS is high even if the other numbers are much improved, as it shows very strong correlations with long term risk, possibly better than any other test including angiography. You could definitely argue than those over 40 or 50 who were or are obese and had evidence of metabolic syndrome should get this checked, even after weight loss. Not covered by medicare in Aus but costs $250 aud and gives very useful information and does not normally ever need to be repeated.It's like $100 here for a coronary CT calcium scan (CAC), if insurance doesn't pay.
It takes about three to five years for the plaque to calcify (enough to be detected on a scan). So a more expensive option is Cardiac CT Angiography (CCTA), which tells you both the past (calcified) and the present (soft plaque).
But most people who are paying out of pocket just do the calcium scan.
Calcium score is a lagging indicator ofr primary prevention . By the time calcium shows up on a scan, you're already well on your way to develop cvd.Agree with this, coronary calcium score is a very good way to determine if statins are needed or not, and is especially useful where calculated risk based on family history, blood pressure , lipids, blood sugar, smoking etc is intermediate, and it will still show changes if those numbers are improved by weight loss, and treatment is an extremely good idea if CCS is high even if the other numbers are much improved, as it shows very strong correlations with long term risk, possibly better than any other test including angiography. You could definitely argue than those over 40 or 50 who were or are obese and had evidence of metabolic syndrome should get this checked, even after weight loss. Not covered by medicare in Aus but costs $250 aud and gives very useful information and does not normally ever need to be repeated.
👏👏👏👏👏Been on GLP-1 for almost 3 years. Lost 1/4 of body weight in 8 months and maintenance since then. Took a while but my doctor stopped my statins today. Never thought it would happen. It took a while but another great NSV.
Yes but that is the point. It is not practical or economic to treat every single person with statins. Treatment is decided by an estimate of absolute risk of MACE or major atherosclerotic cardiovascular events over the next 10 years. Biggest risk by far is age. Then the usual ones family history, smoking, diabetes, blood pressure and lipids. Calculations based on those risk factors are the standard method. Coronary calcium score is an alternate way of assessing risk and is very accurate at predicting future risk, which makes it an excellent tool for deciding if primary prevention is warranted or not.Calcium score is a lagging indicator ofr primary prevention . By the time calcium shows up on a scan, you're already well on your way to develop cvd.
Exactly. It was a self-chosen, self-pay CT calcium scan last August that revealed an 80% occlusion of my LCX and a stent in December that decreased that 80% to 0%. I sent the CAC results to my PCP and she put me on rosuvastatin the same day. LDL went from 141 to 54 between August and December. It was discovered that occlusion is the result of atheriosclerosis.Agree with this, coronary calcium score is a very good way to determine if statins are needed or not, and is especially useful where calculated risk based on family history, blood pressure , lipids, blood sugar, smoking etc is intermediate, and it will still show changes if those numbers are improved by weight loss, and treatment is an extremely good idea if CCS is high even if the other numbers are much improved, as it shows very strong correlations with long term risk, possibly better than any other test
Excellent point. I recently had my calcium CT and guess what? Despite being on a statin for 20 years and keeping my my cholesterol well below even borderline, my calcium score is off the charts. So now I have a cardiologist! Good news? The calcium is in my arterial walls, stabilizing the whole thing. No narrowing. Aced stress test. Hit the gym every day. Only have to see the cardiologist once a year. My LDL is 40 (yes still on a statin, different one at higher strength), total cholesterol <100.Calcium score is a lagging indicator ofr primary prevention . By the time calcium shows up on a scan, you're already well on your way to develop cvd.
Completely agree with this, but there is a greater implication here too. It's very likely OP was put on a statin without evaluating these factors to begin with and purely based on one or two LDL-C (estimated) values from a basic lipid panel alone, as is commonly done in the US and a rather disappointing state of affairs.I think what’s missing here is that LDL alone doesn’t define cardiovascular risk.
The more complete question is: what is this person’s actual risk right now?
That usually involves ApoB, Lp(a), inflammation (hs-CRP), and sometimes CAC.... not just LDL.
So LDL of 90 and stopping statins could be reasonable… or premature.
It depends on factors we’re not seeing discussed: ApoB, LDL-P, Lp(a), inflammation, family history, insulin resistance, CAC, etc.
Without that, it feels like an incomplete picture

Let me preface this by saying that I'm not a doctor and you shouldn't listen to anything resembling medical advice that I might say. It's not medical advice and I'm not qualified to provide that.@tubby
I am seriously interested in your take on my numbers.
I had my CAC on 10/8 and my PCP started me on rosuvastatin on 10/9.
My stent was placed on 12/9.
Again -seriously curious about your take. thx
I should add that I started tirzepatide on June 6, 2025.
SW: 242 lbs, GW 187 lbs reached 11/1/25 and have maintained since.
View attachment 18787
The PREVENT equations estimate absolute 10–year risk for total CVD (PREVENT-CVD), ASCVD (PREVENT-ASCVD) and HF (PREVENT-HF) for adults aged 30–79 years and 30-year risk for total CVD among adults aged 30–59 years. In addition to absolute risk estimates, the calculator provides complementary risk information, including PREVENT–Age and age- and sex-specific 30-year risk percentiles, to help contextualize predicted risk and support clinician–patient discussions.
The American Heart Association PREVENT™ Online Calculator
Welcome to the American Heart Association Predicting Risk of cardiovascular disease EVENTs.professional.heart.org

CVD Risk Estimator Plus - American College of Cardiology
Combining traditional ASCVD risk modeling with modern cardiovascular kidney metabolic (CKM)–inclusive risk equations, CVD Risk Estimator Plus provides clinicians with a comprehensive, personalized cardiovascular disease (CVD) risk assessment.www.acc.org
CVD Risk Estimator Plus computes risk estimates using:
2013 ASCVD Pooled Cohort Equations (PCE), which calculate 10‑year and lifetime risk of atherosclerotic cardiovascular disease using age, sex, race, blood pressure, cholesterol profile, diabetes status, and smoking status.
2023 PREVENT™ Equations, which estimate 10‑ and 30‑year risk for total CVD, ASCVD, and heart failure (HF), incorporating kidney and metabolic health measures such as BMI and estimated glomerular filtration rate (eGFR), and supporting optional predictors including urine albumin‑creatinine ratio (UACR), hemoglobin A1c (HbA1c), and social deprivation index (SDI).
MDCalc uses the 'Hard' coronary Framingham outcomes model, which is intended for use in non-diabetic patients age 30-79 years with no prior history of coronary heart disease or intermittent claudication. This version was selected because it is the most widely applicable to patients without previous cardiac events.
Framingham Risk Score for Hard Coronary Heart Disease Calculator
The Framingham Coronary Heart Disease Risk Score estimates risk of heart attack in 10 years.www.mdcalc.com
See the official Framingham website for additional Framingham risk models.
(2026)
In adults at intermediate risk and select adults at borderline risk with no prior ASCVD, if the decision regarding LLT [lipid-lowering therapy] remains uncertain, a CAC score should be used for further risk stratification and to guide the decision to withhold, postpone, or initiate therapy.
Major Global Coronary Artery Calcium Guidelines (2022)
The figure elucidates an algorithm for suggested CAC scoring and assessing ASCVD risk. CAC = 0 suggests withholding statin therapy, while CAC = 1 to 100 favors lifestyle improvement. CAC = 101 to 400 indicates treatment for individuals >75th percentile, and CAC >400 requires initiation of statin therapy.
Can't speak to those specific links, but I'd take anything the AHA says with a huge grain of salt. They have a history of making claims that seem to benefit industry (pharma and big food) and are scientifically dubious at best and then digging into their positions even after it's clear that claims they've made are flawed (e.g. their long-standing positions on saturated fat and low-carb diets). At a minimum I would check to see if there's a Cochran review article on the same topic and if Cochran supports the AHA position and guidelines or comes to a different conclusion.Regarding calcium CT scoring for intermediate risk:
Risk calculators:
Related guidelines:
Firstly, thank you for the thorough review. I know you're not a doctor nor would I be tempted to consider an anonymous post from a complete stranger as medical advice. That said (mostly as a caveat for others who may read this), I do appreciate your thoughts....with such a rapid weight change in such a short period of time, I'd probably want to see things "settle" for a bit before making any sort of judgement call there....getting to that ratio via a statin is very different than getting to that ratio via lifestyle changes......you probably have many years at which your cardiovascular system was under strain....
Your situation is too complicated for me to have useful advice on, obviously.Not certain where I stand on the statin question. I am not really concerned about it as I also have zero sides from the statin either and I feel better at 62 y.o. than I have in a decade.

I highly recommend the book “Statin Nation” by Dr Malcolm Kendrick He has been a GP for over 25 years and has worked with the European Society of Cardiology.Your situation is too complicated for me to have useful advice on, obviously.
One thing I will add is that there are a large number of studies out there that study the relationship between total cholesterol and all-cause mortality in very large populations (thanks to readily available public health data). A nice trait about all-cause mortality is that it's harder to fake/manipulate than an intermediate marker.
When a statin brings down cholesterol, it's impossible to know how that compares to bringing cholesterol down through other means or how much of a benefit it will actually lead to without studying it. Fortunately, this has been studied in large populations. Unfortunately, those who conducted the (expensive) research are mostly unwilling to share the raw data with groups that might be critical of their work so we're kind of stuck trusting that the pharma-friendly researchers have conducted a fair analysis of the data and haven't applied dubious correction factors or other tricks to skew the data towards a particular conclusion.
What we do know from population-level cholesterol data is that having too low of cholesterol and too high of cholesterol are both associated with significant increases in all-cause mortality. The curve varies by both age and sex. Here is an example of the first curve I could easily find on Google, but there are many studies and they all have somewhat similar results. Choose your favorite if you wish to read more.
View attachment 18807
Some of the low-end risk can be explained by cancer (in late-stage cancer your cholesterol does tend to drop), but that doesn't seem to explain all of it.
And that's why I suggest finding a physician who is skeptical of statin therapy (instead of listening to me) who can better flush out the other side of the equation, enabling you to make a proper objective comparison, since at that point you'll have heard both sides of the story.
I suspect there's at least some truth to the points you raised (or perhaps they're completely correct). There's enough of what I might call suspicious tells in regards to the history of statins to give me pause at the very least.My personal opinion on statins is that it increases insulin resistance and the side effects made running more difficult for me as I was combating my diabetes.