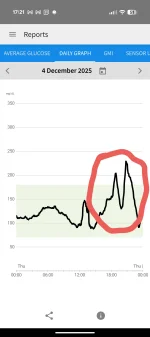
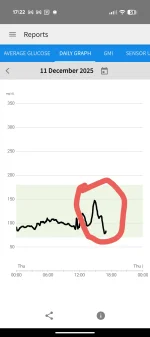
In the past I've controlled my type 2 diabetes with the combination of metformin and a low-carb diet. I stopped the metformin the same day I started the reta, since it would be largely redundant and unnecessary. Since I wear a CGM to keep track of things I have a little more data than most here. Thought I'd share the postprandial response for a meal consisting of roughly one and a half large baked potatoes (which is a great way to create a gigantic blood sugar spike. Here are before and after pics (of the CGM, not me) for anyone curious. The early one would have been with a large amount of butter (which should reduce the magnitude of the spike). The one from today was lightly coated in olive oil (which should make the spike taller). I didn't weigh them out to ensure equivalency or anything, but I find those large spikes don't tend to be strongly portion dependent.
It's striking that within 3 to 4 days, my blood sugar normalized with fasting levels hovering around 80 mg/dL between meals and the glycemic response from any high-glycemic meals has been largely flawless. There was some weight loss in that period, but it wasn't significant enough where I would have anticipated any meaningful difference in blood sugar results based on the small weight change (I'm no stranger to weight fluctuation).
There is a theory (admittedly, kind of fringe) that in some cases type 2 diabetes is ultimately a disorder of excessive glucagon. The thinking goes that because of the excess glucagon, the liver is continually releasing glucose (whether from glycogen stores or gluconeogenesis) at inappropriate times. Specifically, you want your liver to do that a couple hours after a meal (or whenever absorption in the gut slows down to keep food energy flowing), but you want it to stop doing that after you have your next meal and go back to absorbing glucose from the blood instead. If it fails to stop, blood sugar becomes poorly controlled. I have no idea if that theory is right, but since my blood sugar has been well controlled after meals and quickly returned to baseline the last couple days, it does support that idea (since I know my glucagon is currently suppressed at least a small amount).
Very low calories could also partially explain the behavior, but I had ~2500 calories yesterday as well as a late breakfast today, which isn't too far removed from how I would have been eating a week ago. Also when I've previously done extended fasts (typically 2-3 days), they didn't have any sort of carry-over effect like this. As best as I can tell, this is a purely hormonal result.
For those curious, I've had three 1 mg doses and should currently have about 1.5 mg floating around in there (based on half-life calculations).
It's striking that within 3 to 4 days, my blood sugar normalized with fasting levels hovering around 80 mg/dL between meals and the glycemic response from any high-glycemic meals has been largely flawless. There was some weight loss in that period, but it wasn't significant enough where I would have anticipated any meaningful difference in blood sugar results based on the small weight change (I'm no stranger to weight fluctuation).
There is a theory (admittedly, kind of fringe) that in some cases type 2 diabetes is ultimately a disorder of excessive glucagon. The thinking goes that because of the excess glucagon, the liver is continually releasing glucose (whether from glycogen stores or gluconeogenesis) at inappropriate times. Specifically, you want your liver to do that a couple hours after a meal (or whenever absorption in the gut slows down to keep food energy flowing), but you want it to stop doing that after you have your next meal and go back to absorbing glucose from the blood instead. If it fails to stop, blood sugar becomes poorly controlled. I have no idea if that theory is right, but since my blood sugar has been well controlled after meals and quickly returned to baseline the last couple days, it does support that idea (since I know my glucagon is currently suppressed at least a small amount).
Very low calories could also partially explain the behavior, but I had ~2500 calories yesterday as well as a late breakfast today, which isn't too far removed from how I would have been eating a week ago. Also when I've previously done extended fasts (typically 2-3 days), they didn't have any sort of carry-over effect like this. As best as I can tell, this is a purely hormonal result.
For those curious, I've had three 1 mg doses and should currently have about 1.5 mg floating around in there (based on half-life calculations).