
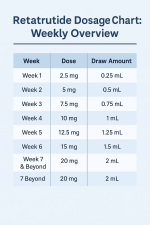
Crazy Dosing Chart
- Thread starter Mr.Tired
- Start date
Trending Topics
Latest Posts
-
 Blood Pressure/Hypertension not dropping
Blood Pressure/Hypertension not dropping- Latest: Foggy-Hollow
-

-

-

-
Members Online
- iKimchi
- Grogu
- lizzai
- Good-Heart6425
- abannon17
- Wafercard
- Katkin
- Prominence
- ShaneH12
- toologic
- Retazempic
- BigPun94
- LipsMel3114
- momo67
- Moocow
- CastleSF
- Determinism
- SpecialTee
- swimmer
- howdyboy
- goose00helton
- desinr-gal
- RedNL
- Juju1334
- benny12b
- bbbaaattt
- ktg123
- ripmygutsout
- Muskott
- fittide
- TeamQic
- Foggy-Hollow
- Davidanza
- joherde11
- jimmybimmy
- malib123
- gulangaloid
- mixderrr
- Ragnar
- Katielobo
- jsopp
- cat_walk
- zasderq
- Brion86
- Cdub100
- Monte2024
- Waclive
- Airborne Daddy
- KCoppo
- the1ronsheik