Yes, there are several reasons why a medication might be prescribed with a
once-a-week dose instead of daily or bi-weekly. The decision often comes down to
effectiveness,
patient convenience, and how the drug is absorbed and processed by the body.
Here are some of the main advantages of a
once-a-week medication:
1. Sustained Release/Long Half-Life:
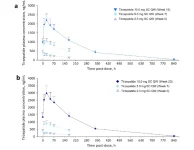
- Some medications are designed to be slow-release or have a long half-life, meaning they stay active in your system for longer periods. This allows for less frequent dosing while still maintaining consistent therapeutic effects.
- For example, some medications used for chronic conditions (like GLP-1 agonists such as tirzepatide) or hormone therapies are formulated to be long-acting, meaning they can work effectively with a weekly dose.
2. Patient Convenience and Adherence:
- Taking medication weekly is often much easier for patients, especially for chronic conditions where long-term adherence is important. Weekly dosing helps improve compliance, as patients are less likely to forget their medication.
- It's easier to remember a weekly dose compared to daily or bi-weekly doses.
3. Reduced Side Effects:
- Some medications cause side effects that may be less pronounced when taken less frequently. By spacing out the doses, the body can avoid high peaks of the drug concentration, potentially reducing side effects like nausea, headaches, or gastrointestinal issues.
- With weekly dosing, the body can adjust to a steady state without overwhelming it with a higher concentration that daily doses might cause.
4. Lower Peaks and Troughs:
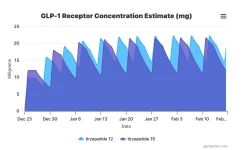
- Some medications have peaks (high concentration) and troughs (low concentration) in their effect when taken daily. A weekly dose can allow for a smoother, more consistent effect by flattening the peaks and troughs, ensuring the drug stays active in the system at a steady level over time.
5. Specialized Formulations:
- Some drugs are specially formulated to be slow-release, such as extended-release tablets or injectables. These formulations gradually release the medication over time, making it effective for longer durations.
- For example, some hormonal therapies and biologic injections are designed to provide therapeutic levels with minimal fluctuations, which works well with weekly dosing.
6. Cost and Insurance Benefits:
- In some cases, having a weekly dose can be more cost-effective for both the patient and the healthcare system, as it reduces the number of prescriptions or visits to a healthcare provider. It's more convenient and can be more affordable than daily or bi-weekly therapies.
Examples of Weekly Medications:
- GLP-1 Agonists (e.g., tirzepatide, semaglutide) – Often prescribed weekly for diabetes or weight loss. These drugs have long half-lives, allowing for less frequent administration.
- Hormonal Therapies (e.g., testosterone replacement) – Some testosterone therapies are designed to be injected weekly, as they have a long-lasting effect in the body.
- Biologic Drugs – Medications for autoimmune conditions like Rheumatoid Arthritis (e.g., Humira) may be prescribed on a weekly or bi-weekly basis due to their prolonged effects.
In short, the decision to prescribe
once-weekly medication is often based on maximizing
effectiveness,
convenience, and
patient compliance while minimizing
side effects.