I think that assumption is too simplistic. Wanting to be “thin” is not the best frame; preserving a lean, strong physique is a better goal during weight loss.
Peptides associated with growth signalling do not automatically make a woman bulky. That depends on the full context: dose, diet, training, genetics, and total energy balance.
If you’re on a GLP, I’d actually be more concerned about muscle loss than “bulking.” In that context, a GH secretagogue may help support lean mass retention, especially if protein intake is below 1g/lb of ideal body weight and resistance training is not in place.
I can say from personal experience that GH secretagogues do not automatically make a woman bulky. I eat 80–120 g of protein daily, have taken Tesa (1 mg)/Ipa (200 mcg) nightly this past quarter, and have been very satisfied with the results—lean, athletic, and far from bulky.
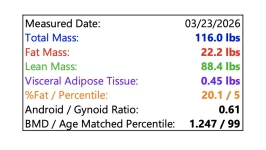
Included: last week’s DEXA and my smart scale data as a real-world example.