I think you're confused about what harm reduction means. The purpose of this forum is harm reduction. We all take risks, but encouraging reckless behavior won't be tolerated. That kind of dose escalation can easily put someone in the hospital or worse.It's not the most popular opinion(especially here), but RESULTS are the goal, harm reduction is and always will be priority 2.
No matter what anyone here or anywhere says, If you're injecting experimental peptides, not even considering they come from the chinese gray market of all fkn places, you're willing to at least risk a LITTLE harm if it will get you the RESULTS you want.
This guy seems like the average newcomer in SSA's Discord(You guys should take a peek in there when bored, some of those idiots are HILARIOUS) who is lacking general understandings of Half-lifes(lives? nah),and probably reta itself. For the love of god hes pinning subq into his THIGH. he probably just needs to fuck himself up a little bit(in a clean and safe ish and reparable way) and he'll learn his lesson and start reading. He's already taken the first step by coming here and opening himself up to verbal abusein exchange for (if hes lucky) some good advice.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Drugs for reta side effects
- Thread starter diogenes
- Start date
PackmanJohnny
GLP-1 Apprentice
Yeah I totally could be conflating Harm reduction with Harm avoidance(Risk aversion? I need sleep, finals week).I think you're confused about what harm reduction means. The purpose of this forum is harm reduction. We all take risks, but encouraging reckless behavior won't be tolerated. That kind of dose escalation can easily put someone in the hospital or worse.
I've been that kid running 400mgs of DNP because the info sources I had access to were not good, a large percent of people in this space become a lot more careful after they touch the stove once or twice and thats just how they learned. When you know better, you do better.
Hopefully he gleans some info and gets himself educated. I've never really thought about the consequences of OD'ing on GLPs, because that would require some TENACIOUS stupidity, but the deeper I get into this world I do find that bar creeping lower and lower.
peptidepower77
GLP-1 Enthusiast
What's wrong with pinning subq in your thigh? That's a pretty standard place on the Mounjaro docs, for testosterone replacement etc.It's not the most popular opinion(especially here), but RESULTS are the goal, harm reduction is and always will be priority 2.
No matter what anyone here or anywhere says, If you're injecting experimental peptides, not even considering they come from the chinese gray market of all fkn places, you're willing to at least risk a LITTLE harm if it will get you the RESULTS you want.
This guy seems like the average newcomer in SSA's Discord(You guys should take a peek in there when bored, some of those idiots are HILARIOUS) who is lacking general understandings of Half-lifes(lives? nah),and probably reta itself. For the love of god hes pinning subq into his THIGH. he probably just needs to fuck himself up a little bit(in a clean and safe ish and reparable way) and he'll learn his lesson and start reading. He's already taken the first step by coming here and opening himself up to verbal abusein exchange for (if hes lucky) some good advice.
Attachments
PackmanJohnny
GLP-1 Apprentice
What's wrong with pinning subq in your thigh? That's a pretty standard place on the Mounjaro docs, for testosterone replacement etc.
I could totally be of the mark, Ive only pinned sema as far as GLP's go - I guess some people dont experience as much PIP as others, but Ive learned to avoid areas that involve a lot of movement. most Subq injections can be done in the stomach as easily as anywhere else.
Its also probably not as big of a risk with Subq as IM, but Ive seen a lot of medical warnings about needles and thighs - potential for nerve damage and whatnot. both of my last two doctors instructed the same to me.
peptidepower77
GLP-1 Enthusiast
I don't see why, my thigh has plenty of skin + fat on it. Regardless, subq is only supposed to break through to just under the final layer of the skin. It's why most subq needles are only 5mm. If you're using a 8-12mm needle that you brought mistakenly I can see it maybe hurting. But for even practical reasons (like being better able to visualize where I'm going to pin it), my thighs are way easier than my stomach for me. Lots of people report less side effects as well (I haven't experienced that), but that could just be placebo so who knows.I could totally be of the mark, Ive only pinned sema as far as GLP's go - I guess some people dont experience as much PIP as others, but Ive learned to avoid areas that involve a lot of movement. most Subq injections can be done in the stomach as easily as anywhere else.
Its also probably not as big of a risk with Subq as IM, but Ive seen a lot of medical warnings about needles and thighs - potential for nerve damage and whatnot. both of my last two doctors instructed the same to me.
Thigh is usually not recommended for IM anymore because ventroglute and lateral delt are so much better. But its fine for subQ, especially if you're not very lean.I could totally be of the mark, Ive only pinned sema as far as GLP's go - I guess some people dont experience as much PIP as others, but Ive learned to avoid areas that involve a lot of movement. most Subq injections can be done in the stomach as easily as anywhere else.
Its also probably not as big of a risk with Subq as IM, but Ive seen a lot of medical warnings about needles and thighs - potential for nerve damage and whatnot. both of my last two doctors instructed the same to me.
diogenes
GLP-1 Apprentice
Much of it isn't responsive to my actual question, but what is seems pretty good, and I'm grateful for it.It's not the most popular opinion(especially here), but RESULTS are the goal, harm reduction is and always will be priority 2.
No matter what anyone here or anywhere says, If you're injecting experimental peptides, not even considering they come from the chinese gray market of all fkn places, you're willing to at least risk a LITTLE harm if it will get you the RESULTS you want.
This guy seems like the average newcomer in SSA's Discord(You guys should take a peek in there when bored, some of those idiots are HILARIOUS) who is lacking general understandings of Half-lifes(lives? nah),and probably reta itself. For the love of god hes pinning subq into his THIGH. he probably just needs to fuck himself up a little bit(in a clean and safe ish and reparable way) and he'll learn his lesson and start reading. He's already taken the first step by coming here and opening himself up to verbal abusein exchange for (if hes lucky) some good advice.
I don't appreciate the contemptuous, peacocking digressions, kind of like Linux USENET in the late '90s ("RTFM!!1"; "n00b!!"). I rarely post on forums, and I'd hoped the culture had matured. Apparently not.
As far as I've read, subq injection into the anterolateral thigh is fine, especially with a fatty thigh, as I have. Nothing I can find in published protocols for GLP-1 drugs mandates a specific injection site. Papers report that some patients prefer the thigh, with no shade cast on this site. From what sources I can find, thigh might yield slightly less/slower availability than abdomen, but the difference is regarded as insignificant.
If there are sources I've missed that indicate otherwise, I'd be curious to learn about them and change my injection site accordingly.
diogenes
GLP-1 Apprentice
Interestingly, my resting heart rate wasn't higher than normal, even when I was most agitated. Still, if I ever experience elevated heart rate, I'll consider atenolol, of which I happen to have some. Thanks!I take just a 1/4 dose of a cardio selective beta blocker and it seems to help. Same thing if stacking with T3 or T4. Its hard to sleep when your pulse rate is though the roof!
If you like natural, a few Hawthorn Berry capsules can be surprisingly effective as well.
DR.D.
GLP-1 Novice
🚫No Source Discussion🚫
Interestingly, my resting heart rate wasn't higher than normal, even when I was most agitated. Still, if I ever experience elevated heart rate, I'll consider atenolol, of which I happen to have some. Thanks!
Yes sir, same one I choose also. 12.5mg is all it takes for me to take the edge off, and I just take it situationally, maybe once or twice a week as needed.
DR.D.
GLP-1 Novice
🚫No Source Discussion🚫
Betaine for backed up? How much?Melatonin for sleep
Fibre for washroom
And betaine for backed up
Cenn_Buie
Recently Joined
🚫No Source Discussion🚫
Much of it isn't responsive to my actual question, but what is seems pretty good, and I'm grateful for it.
I don't appreciate the contemptuous, peacocking digressions, kind of like Linux USENET in the late '90s ("RTFM!!1"; "n00b!!"). I rarely post on forums, and I'd hoped the culture had matured. Apparently not.
As far as I've read, subq injection into the anterolateral thigh is fine, especially with a fatty thigh, as I have. Nothing I can find in published protocols for GLP-1 drugs mandates a specific injection site. Papers report that some patients prefer the thigh, with no shade cast on this site. From what sources I can find, thigh might yield slightly less/slower availability than abdomen, but the difference is regarded as insignificant.
If there are sources I've missed that indicate otherwise, I'd be curious to learn about them and change my injection site accordingly.
What you are reading is correct. Eli Lilly looked into this with tirzepatide recently. Link to clinical trial: https://clinicaltrials.gov/study/NCT04050670?tab=results#limitations-and-caveats
Summary:
- abdomen gets you a bit more tirzepatide (112000 h * ng/mL) versus arm (111000 h * ng/mL) or thigh (106000 h * nh/mL), but it's not a big difference; Outcome Measure 1
- abdomen gets you a noticeably higher peak concentration of tirzepatide (603 ng/mL) than upper arm (556 ng/mL), which is in turn higher than thigh (520 ng/mL); Outcome Measure 2
- abdomen also gets you noticeably more side effects (68.5%) than upper arm (57.41%) or thigh (43.40%), particularly for nausea (21 events vs. 12 vs. 12) and vomiting (10 events vs. 10 vs. 4); Adverse Events
diogenes
GLP-1 Apprentice
Interesting. The geometric mean of the %gCV (or do we use arithmetic?) for all 3 injection sites is like 5x the AUC concentration, so I'm not even sure we can conclude it matters. That's a lot more noise than signal.What you are reading is correct. Eli Lilly looked into this with tirzepatide recently. Link to clinical trial: https://clinicaltrials.gov/study/NCT04050670?tab=results#limitations-and-caveats
Summary:
Since they used the same people on all arms of the study, the effect of variation between people (i.e. some people are more sensitive to tirzepatide than others) should be minimized.
- abdomen gets you a bit more tirzepatide (112000 h * ng/mL) versus arm (111000 h * ng/mL) or thigh (106000 h * nh/mL), but it's not a big difference; Outcome Measure 1
- abdomen gets you a noticeably higher peak concentration of tirzepatide (603 ng/mL) than upper arm (556 ng/mL), which is in turn higher than thigh (520 ng/mL); Outcome Measure 2
- abdomen also gets you noticeably more side effects (68.5%) than upper arm (57.41%) or thigh (43.40%), particularly for nausea (21 events vs. 12 vs. 12) and vomiting (10 events vs. 10 vs. 4); Adverse Events
It looks like the tests conclude that neither arm nor thigh is inferior, but they don't assess if the observed difference in AUC concentration, C_max, or side effect rate is significant.
My guess is that the differences are not statistically significant (except for maybe nausea/vomitting), and we should presume that changing the injection site doesn't matter.
No?
Yes, this is the correct conclusion. Is there a difference, probably. But it's not enough to matter for the majority of people.Interesting. The geometric mean of the %gCV (or do we use arithmetic?) for all 3 injection sites is like 5x the AUC concentration, so I'm not even sure we can conclude it matters. That's a lot more noise than signal.
It looks like the tests conclude that neither arm nor thigh is inferior, but they don't assess if the observed difference in AUC concentration, C_max, or side effect rate is significant.
My guess is that the differences are not statistically significant (except for maybe nausea/vomitting), and we should presume that changing the injection site doesn't matter.
No?
MsGizmo
GLP-1 Enthusiast
Quicker weight loss isn't necessarily the best thing for your body. I myself need to lose nearly 200 pounds, so I absolutely understand the appeal of quick results. Triggering more severe side effects isn't worth it though. Especially when some of them can be very serious. Personally I want a slower loss to minimize loose skin as much as I can. There are many other reasons but I think the one that you would likely be most interested in .. rapid weight loss damages your metabolism and I haven't seen a single bit of research on how that can be fixed.I figured the quicker weight loss was worth it.
ocuzuc
GLP-1 Apprentice
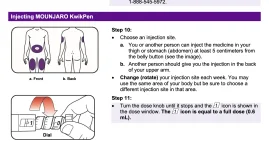
I only pin in my thighs, subq. I was doing belly injections as that was easy and recommend for Mounjaro auto-injectors. I got heavy nausea for 2 days. My doctor gave me an Rx for Zofran, but isn’t in general a fan of treating drug side effects with another drug, it can become an endless cycle. He suggested using the thighs, as it is absorbed slower. The glutes would be the slowest, and would probably fine, but it is not an approved injection site for Mounjaro. And it’s harder to self inject back there. But guess what? That simple change of injection location to the thigh significantly reduced the amount and duration of the nausea. Even tho I rarely get nausea now, I still only do thighs.I don't see why, my thigh has plenty of skin + fat on it. Regardless, subq is only supposed to break through to just under the final layer of the skin. It's why most subq needles are only 5mm. If you're using a 8-12mm needle that you brought mistakenly I can see it maybe hurting. But for even practical reasons (like being better able to visualize where I'm going to pin it), my thighs are way easier than my stomach for me. Lots of people report less side effects as well (I haven't experienced that), but that could just be placebo so who knows.
But, but, overthinking every little thing!Yes, this is the correct conclusion. Is there a difference, probably. But it's not enough to matter for the majority of people.

Calm Logic
GLP-1 Specialist
Better than the alternative, haha.

Cenn_Buie
Recently Joined
🚫No Source Discussion🚫
They don't assess if the observed difference in AUC concentration, C_max, or side effect rate is significant.
Exactly. The study was designed as a non-inferiority trial. If non-inferiority criteria was met, then they would have spent the $$$ needed to run a proper trial with more patients, but since the 3 injection sites were non-inferior, they didn't bother going any further. You could say that there is a signal towards slightly higher peak AUC and worse side effect profile with abdominal injection but we can't draw a definitive conclusion one way or another.Is there a difference, probably. But it's not enough to matter for the majority of people.
My takeaway is that we should all just rotate sites to see what works best for us. What is clear is that each participant had different results with different injection sites. In my case, if I inject in the thigh I don't have nearly as much fatigue on day 2-3 so I'm going to keep doing that.
diogenes
GLP-1 Apprentice
Good point.Quicker weight loss isn't necessarily the best thing for your body. I myself need to lose nearly 200 pounds, so I absolutely understand the appeal of quick results. Triggering more severe side effects isn't worth it though. Especially when some of them can be very serious. Personally I want a slower loss to minimize loose skin as much as I can. There are many other reasons but I think the one that you would likely be most interested in .. rapid weight loss damages your metabolism and I haven't seen a single bit of research on how that can be fixed.
I should have been clearer. I hope to lose 65lb (270 -> 205) in 52-72 weeks. So a ~25% reduction. I don't really care about speed of loss, but I want to maximize the probability of success. At the highest dose (15mg) in the tirz trials paper, only 39.7% of participants achieved 25% by week 72. But in the phase 2 reta paper, 48% of those taking the highest dose hit 25% by week 48—and from the graph it looks like far more (I'd guess 70%+) would have had the trials lasted to week 72 like tirz.
That's a big difference. It's the difference between "I can almost certainly get non-obese," and "I can almost certainly get non-overweight." To me, it's worth some uncertainty and some side effects to get the latter.
As far as speed, Do you think my ambitions raise concern about metabolic damage, and if so what metabolic damage, and how might I measure it?
You're approaching it with the right mindset. That speed of loss is definitely healthy and more than achievable.Good point.
I should have been clearer. I hope to lose 65lb (270 -> 205) in 52-72 weeks. So a ~25% reduction. I don't really care about speed of loss, but I want to maximize the probability of success. At the highest dose (15mg) in the tirz trials paper, only 39.7% of participants achieved 25% by week 72. But in the phase 2 reta paper, 48% of those taking the highest dose hit 25% by week 48—and from the graph it looks like far more (I'd guess 70%+) would have had the trials lasted to week 72 like tirz.
That's a big difference. It's the difference between "I can almost certainly get non-obese," and "I can almost certainly get non-overweight." To me, it's worth some uncertainty and some side effects to get the latter.
As far as speed, Do you think my ambitions raise concern about metabolic damage, and if so what metabolic damage, and how might I measure it?
Something that might make you feel better as well, most people that put effort into starting moderate weight training, cardio, and a healthy diet typically get way better results than the average. I lost over 40% of my body weight (first half with tirz then finished with reta, and its not unusual.
Last edited:
chmuse
Public Nuisance 🦜🐧🦅🦚🦃🦢🐓🦆🦉
He just started his fox journey.I miss @raw_oyster_eater. He would try anything once.
chmuse
Public Nuisance 🦜🐧🦅🦚🦃🦢🐓🦆🦉
All I changed was my diet, and I lost 20% in six months on sema. I think it varies wildly by person, because I am absolutely still a couch potato.You're approaching it with the right mindset. That speed of loss is definitely healthy and more than achievable.
Something that might make you feel better as well, most people that put effort into starting moderate weight training, cardio, and a healthy diet typically get way better results than the average. I lost over 40% of my body weight (first half with tirz then finished with reta, and its unusual.
ocuzuc
GLP-1 Apprentice
I lost 75lbs (255->180) on tirz alone in 10 months. but mine is technically side effect as my objective was to get my blood glucose back down to normal. fasting was 137 with an a1c of 6.3. now it’s 74 and 5.2 as well after the same 10 months. but I was a slow responder and I think i only lost 8 lbs and no glucose change in the first 3 months. yet i got many of the bad side effects: super nausea, massive constipation, crushing fatigue. It was some much I wanted to stop, more than once and was just going to take metformin for the rest of my life, but my doctor kept encouraging me to stick with it. the selling point was he kept referring to the 94% cure rate for pre-diabetes from tirz, “we never see cure rates like that in medicine!” he kept saying. but eventually it kicked in around month 4 to 5 for me.Good point.
I should have been clearer. I hope to lose 65lb (270 -> 205) in 52-72 weeks. So a ~25% reduction. I don't really care about speed of loss, but I want to maximize the probability of success. At the highest dose (15mg) in the tirz trials paper, only 39.7% of participants achieved 25% by week 72. But in the phase 2 reta paper, 48% of those taking the highest dose hit 25% by week 48—and from the graph it looks like far more (I'd guess 70%+) would have had the trials lasted to week 72 like tirz.
That's a big difference. It's the difference between "I can almost certainly get non-obese," and "I can almost certainly get non-overweight." To me, it's worth some uncertainty and some side effects to get the latter.
As far as speed, Do you think my ambitions raise concern about metabolic damage, and if so what metabolic damage, and how might I measure it?
MsGizmo
GLP-1 Enthusiast
Taking the time to allow your body to adjust to gradually higher doses would only prolong the process by a few weeks at most .. but if you aren't worried about how much time it takes then you should absolutely take your time upping your doses slowly. Just because the people in the study didn't get to a 25% weight loss by 72 weeks on a lower dose does not mean that they would not EVENTUALLY get there. I am taking semaglutide, the glp1 with the least impressive numbers according to the studies .. but there are plenty of people out there telling their stories of losing much more weight than they were predicted to lose using it. Will I be one of those stories? I don't know. But as long as I continue to lose weight with it I will keep using it.Good point.
I should have been clearer. I hope to lose 65lb (270 -> 205) in 52-72 weeks. So a ~25% reduction. I don't really care about speed of loss, but I want to maximize the probability of success. At the highest dose (15mg) in the tirz trials paper, only 39.7% of participants achieved 25% by week 72. But in the phase 2 reta paper, 48% of those taking the highest dose hit 25% by week 48—and from the graph it looks like far more (I'd guess 70%+) would have had the trials lasted to week 72 like tirz.
That's a big difference. It's the difference between "I can almost certainly get non-obese," and "I can almost certainly get non-overweight." To me, it's worth some uncertainty and some side effects to get the latter.
As far as speed, Do you think my ambitions raise concern about metabolic damage, and if so what metabolic damage, and how might I measure it?
As far as metabolic damage prevention .. I don't know of any way to measure it. All I can say to that is what I've been told .. focus on getting enough protein, fiber and water. Maybe take a daily multivitimin too.
FlowerFairy
GLP-1 Enthusiast
His Fox journey?He just started his fox journey.
FlowerFairy
GLP-1 Enthusiast
It’s not just “aggressive.” It’s reckless. What part of “it takes 4 weeks to reach full effect” do you not understand? Titrating up faster isn’t aggressive, it’s just plain stupid.I prefer the term "aggressive," but yes I'm aware the phase 2 trials started at much lower doses. I'll give it a rest for a bit and restart more gently.
FlowerFairy
GLP-1 Enthusiast
If it’s contemptuous to you, that could be a hint you are not acting in your own best interests. If having knowledge and sharing it is “peacocking,” then why are you here? You could go to Meso and get uneducated poor advice more in line with your thinking.Much of it isn't responsive to my actual question, but what is seems pretty good, and I'm grateful for it.
I don't appreciate the contemptuous, peacocking digressions, kind of like Linux USENET in the late '90s ("RTFM!!1"; "n00b!!"). I rarely post on forums, and I'd hoped the culture had matured. Apparently not.
As far as I've read, subq injection into the anterolateral thigh is fine, especially with a fatty thigh, as I have. Nothing I can find in published protocols for GLP-1 drugs mandates a specific injection site. Papers report that some patients prefer the thigh, with no shade cast on this site. From what sources I can find, thigh might yield slightly less/slower availability than abdomen, but the difference is regarded as insignificant.
If there are sources I've missed that indicate otherwise, I'd be curious to learn about them and change my injection site accordingly.
FlowerFairy
GLP-1 Enthusiast
What good is giving him good advice when he has made it clear he prefers ill advised shortcuts to actual knowledge? Because apparently facts = “peacocking.” Does not sound like he plans to listen to any good advice- he discounted it al with, “they didn’t tell me what I asked for.” No we did not- we told you what you need to do to be safe. But hey- he already poisoned himself with a Reta overdose- let’s throw more drugs into the mix! Then when he titrates up to 20 mg like the other one, the ED will have no idea how to help him. 🙄It's not the most popular opinion(especially here), but RESULTS are the goal, harm reduction is and always will be priority 2.
No matter what anyone here or anywhere says, If you're injecting experimental peptides, not even considering they come from the chinese gray market of all fkn places, you're willing to at least risk a LITTLE harm if it will get you the RESULTS you want.
This guy seems like the average newcomer in SSA's Discord(You guys should take a peek in there when bored, some of those idiots are HILARIOUS) who is lacking general understandings of Half-lifes(lives? nah),and probably reta itself. For the love of god hes pinning subq into his THIGH. he probably just needs to fuck himself up a little bit(in a clean and safe ish and reparable way) and he'll learn his lesson and start reading. He's already taken the first step by coming here and opening himself up to verbal abusein exchange for (if hes lucky) some good advice.
MsGizmo
GLP-1 Enthusiast
Well .. because not only is there a chance that he will listen to a kinder voice gently pointing him in the right direction .. there are going to be other people reading this thread who can benefit not only from his mistakes but our advice on how to deal with them after the fact if they have already done the same thing.What good is giving him good advice when he has made it clear he prefers ill advised shortcuts to actual knowledge?
I have mentioned in several other posts that I completely understand the despair of obesity and desperation to lose weight. I mean I let a doctor cut out 80% of my stomach hoping that it would help me. It sounds completely insane if I allow myself to think about it too much. I have been obese for more than 25 years. So I get it. Now after all these years the idea of taking these shots and having the fat just melt away. Well .. that sure is a powerful dream isn't it? But as much as I would love to magically return to the size 6 I used to be before I had kids I also don't want to die trying to get there.