bluefootedboobie
GLP-1 Novice
🚫No Source Discussion🚫
Has anyone here successfully overcome a retatrutide plateau, that couldn't be overcome by increasing the dose?
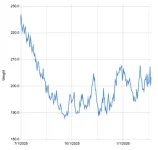
I dropped approximately 30 lbs of fat in my first three months taking reta, titrating up to 6 mg per week. I'd had food noise / food addiction all my life, but reta was finally the cure that got my brain to say hey, I'm just not interested in overeating. The reta also manifested with lower alcohol. I was a problem drinker, but found myself drinking a LOT less.
After those three months though, it was like my brain hit a wall and the mental effects of reta completely stopped working. Cravings returned and I again started having no trouble putting down 7 to 8000 calories in a day. The desire to drink returned eventually as well.
Gastric motility appears to have been impacted as well. For those three months when reta was working, it felt like my stomach was constantly full, to the point that my esophagus was "backed up" and I couldn't physically cram food down my throat. I believe my motility remains a bit slower than it was prior to reta, but unlike before when it was 1000% crystal clear, I now have no trouble always fitting food in.
I've since titrated up to 12 mg of reta per week in an attempt to overcome the plateau, but it hasn't had any affect whatsoever. For several months now, in short, it simply feels like reta no longer works.
For what it's worth, and for those who haven't heard -- this plateau-ing seems to be very individualized. Some folks experience it, and many don't.
The question:
What is the solution for this?
Has anyone had success with reta for a period, had it lose its effectiveness, then regained it?
If so, how did you do it? Perhaps by taking a sustained break? If so, for how long?
Or perhaps the introduction of cagrilintine? Or tesofensine?
Any and all advice would be greatly appreciated.
I dropped approximately 30 lbs of fat in my first three months taking reta, titrating up to 6 mg per week. I'd had food noise / food addiction all my life, but reta was finally the cure that got my brain to say hey, I'm just not interested in overeating. The reta also manifested with lower alcohol. I was a problem drinker, but found myself drinking a LOT less.
After those three months though, it was like my brain hit a wall and the mental effects of reta completely stopped working. Cravings returned and I again started having no trouble putting down 7 to 8000 calories in a day. The desire to drink returned eventually as well.
Gastric motility appears to have been impacted as well. For those three months when reta was working, it felt like my stomach was constantly full, to the point that my esophagus was "backed up" and I couldn't physically cram food down my throat. I believe my motility remains a bit slower than it was prior to reta, but unlike before when it was 1000% crystal clear, I now have no trouble always fitting food in.
I've since titrated up to 12 mg of reta per week in an attempt to overcome the plateau, but it hasn't had any affect whatsoever. For several months now, in short, it simply feels like reta no longer works.
For what it's worth, and for those who haven't heard -- this plateau-ing seems to be very individualized. Some folks experience it, and many don't.
The question:
What is the solution for this?
Has anyone had success with reta for a period, had it lose its effectiveness, then regained it?
If so, how did you do it? Perhaps by taking a sustained break? If so, for how long?
Or perhaps the introduction of cagrilintine? Or tesofensine?
Any and all advice would be greatly appreciated.